Ultrasound anatomy:
- Epidermis/Dermis: Single echogenic layer.
- Subcutaneous fatty tissue: Generally hypoechoic with hyperechoic fibrous septa.
- Fascial planes: Hyperechoic.
- Muscle: Striated appeareance. (1)
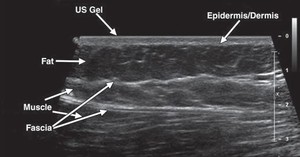
Fig. 1: Ultrasound anatomy
1st.
case: 48 year old male with acute arm swelling after venipuncture.
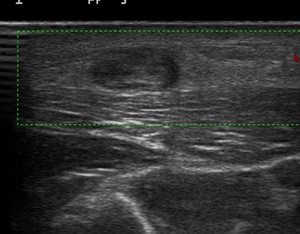
Fig. 2: Short-axis view of a thrombosed and inflamed vein. The sonographic findings show a noncompressible vein with an anechoic thrombus within the lumen, vessel wall thickening, and lack of color Doppler flow.
References: Department of Radiology, Hospital Vall d'Hebron
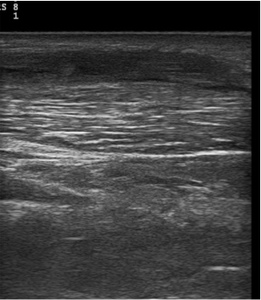
Fig. 3: Cellulitis. Transvers sonogram shows diffuse thickening and increased echogenicity of the skin and subcutaneous tissues and hypoechoic strands between the hyperechoic fat.
- Infection of the skin and subcutaneous tissue.
- Main role is the detection of occult abscess.
- US can assess patency of venous structures.
- US findings are not pathognomonic (e.g heart failure,
lymphedema).
- Findings: Thickening and increased echogenicity of the subcutaneous soft tissue,
hypoechoic strands between the hyperechoic fat and connective tissue (cobblestone appearance in severe extensive cellulitis),
Hyperemia with color Doppler. (2)
2nd.
Case: 45 year old woman who had axillary lymph node dissection.
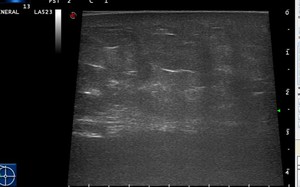
Fig. 4: Sonogram reveals poorly defined, predominantly echogenic subcutaneous mass and skin thickening .
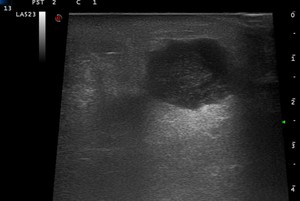
Fig. 5: Abscess. Sonogram shows an hypoechoic complex fluid collection with well-circumscribed borders and hyperechoic surrounding structures.
References: Department of Radiology, Hospital Vall d'Hebron
- The majority of cases are caused by s.aureus.
- Ultrasonographic appearance is highly variable.
Usually spherical with irregular/lobulated and well or poorly defined bordes.
- Contents may be anechoic,
hypoechoic,
hyperechoic.
- Peripheral Doppler signal.
- Typically shows posterior acoustic enhancement.
- Oftenly associated cellulitis.
- Possibility to perform US-guided aspiration (treatment or study). (2,3)
3rd.
case: 77 year old men with lung cancer and acute generalized swelling in chest.
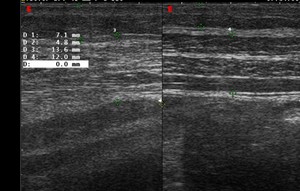
Fig. 6: Comparative ultrasound showing thickening of the muscular wall and subcutaneous tissue, as well as loss of normal echostructure.
References: Department of Radiology, Hospital Vall d'Hebron

Fig. 7: CT axial image demonstrates the edema of the subcutaneous tissue.
References: Department of Radiology, Hospital Vall d'Hebron
- EDEMA OF THE SUBCUTANEOUS TISSUE
- Linear fluid infiltration of soft tissues.
- Multiple etiology: CKD,
CHF,
Shock...
- Not well defined collections are observed.
4th.
case: 21 year old man with recent pastmedical history of politraumatism.
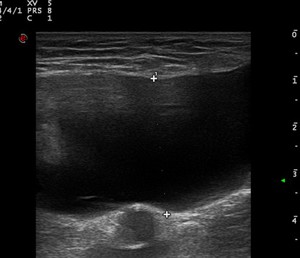
Fig. 8: Hypoechoic and homogeneous fluid collection with well-defined margins.
References: Department of Radiology, Hospital Vall d'Hebron
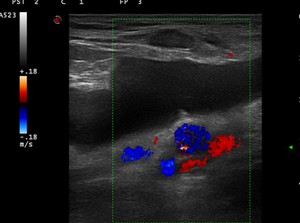
Fig. 9: Fusiform anechoic fluid collection with smooth margins, which was compressible and had no intrinsic flow on color Doppler imaging.
References: Department of Radiology, Hospital Vall d'Hebron

Fig. 10: CT axial image show hypodense collection within deep subcutaneous tissues.
References: Department of Radiology, Hospital Vall d'Hebron
- Traumatic separation of subcutaneous tissue from the underlying fascia with accumulation of blood,
lymph,
fat,
and debris.
- Most frequently over the greater trochanter,
also prepatellar.
- Hypoechoic or anechoic between the deep fat and overlying fascia.
- Percutaneous US-guided aspiration is possible.(4)
5th.
case: 73 year old man with LUQ pain with swelling.
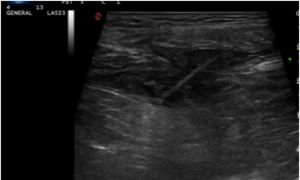
Fig. 11: Soft-tissue ultrasound imaging reveals a foregin body surrounded by a hypoechoic halo of edema.
References: Department of Radiology, Hospital Vall d'Hebron
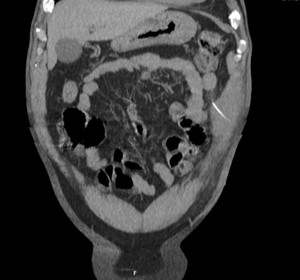
Fig. 12: CT coronal scan showing a foregin body transversely located at the muscle in the anterior abdominal wall.
References: Department of Radiology, Hospital Vall d'Hebron
- SOFT TISSUE INFECTION SECONDARY TO MIGRATED FOREIGN BODY "FISH BONE".
- Inflammatory response that results in encapsulation or expel of foreign body.
- US findings: Poorly defined and hypoechogenic masses typically with associated cellulitis.
All foreign bodies are hyperechoic,
some of them have a surrounding hypoechoic halo of edema.
- Sometimes it is posible to identify the foreign body.(1).
6th case: 30 year old man with right lower quadrant paind,
without fever and past medical history of HIV.
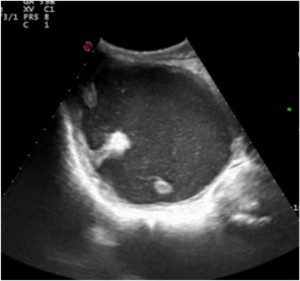
Fig. 13: Soft-tissue ultrasound imaging reveals a foregin body surrounded by a hypoechoic halo of edema.
References: Department of Radiology, Hospital Vall d'Hebron
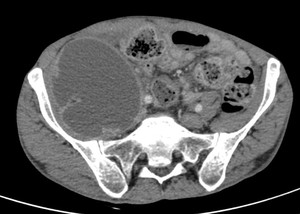
Fig. 14: CT scan confirming an abscess in the enlarged right psoas.
References: Department of Radiology, Hospital Vall d'Hebron
- Primary (probably haematogenous spread) usually S.aureus and in patiens with immunocompromised state,
or secondary due to infection from and adjacent organ.
- Clasical triad: Fever,
back pain,
limp.
- More often right than left.
- Percutaneous drainage is recommended as a part of treatment.
7th.
case: 80 year old woman with acute painful mass in anterior forearm.

Fig. 15: Ultrasound demonstrates a large heterogeneous, intramuscular lesion representing an hematoma.
References: Department of Radiology, Hospital Vall d'Hebron
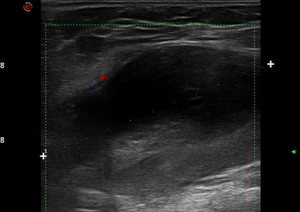
Fig. 16: Intramuscular haematoma. Ultrasound imaging shows an anechoic lesion with well-circumscribed margins and lack of color Doppler flow.
References: Department of Radiology, Hospital Vall d'Hebron
- Variable US appearances,
tipically round or oval with sharply margins.
- Acute phase: Well circumscribed and anechoic.
- Subacute phase: More hyperechoic and heterogeneous.
- Late-chronic phase: Mural nodular,
internal septations,
liquefaction,
anechoic.(1,5).
8th case: 57 year old man with right rib cage pain and swelling.
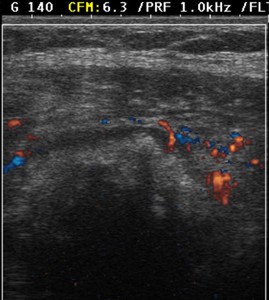
Fig. 17: Rib metastasis. Ultrasound shows bone destruction and mass formation.
References: Department of Radiology, Hospital Vall d'Hebron
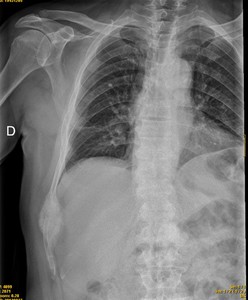
Fig. 18: CXR shows an expansile mass in the rib.
References: Department of Radiology, Hospital Vall d'Hebron
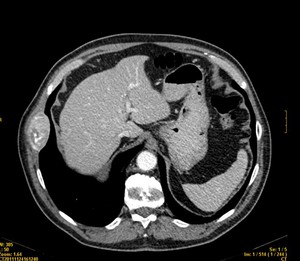
Fig. 19: CT scan shows an expansile lytic rib lesion.
References: Department of Radiology, Hospital Vall d'Hebron
- BONE METASTASES FROM ADENOCARCINOMA OF UNKNOWN PRIMARY SITE.
9th case: 33 year old man with right orchitis.
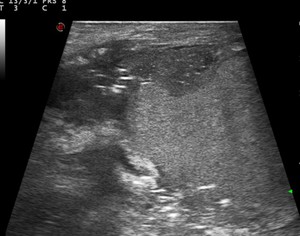
Fig. 20: Ultrasound images show echogenic foci within the scrotal wall suggestive of gas within the scrotum.
References: Department of Radiology, Hospital Vall d'Hebron
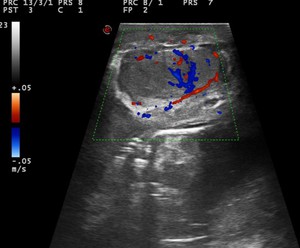
Fig. 21: Ultrasound imaging of the scrotum showed marked thickening of the scrotal wall with hyperemia of the scrotum seen as increased vascularity on colour Doppler ultrasound imaging.
References: Department of Radiology, Hospital Vall d'Hebron

Fig. 22: Ultrasound demonstrates thickened scrotal wall with dirty acoustic shadowing gas foci in scrotum.
References: Department of Radiology, Hospital Vall d'Hebron
- Necrotisin fasciitis of the perineum.
- Pain disproportionate to the severity of cellulitis.
- Group A streptococci are the most common offending organisms.
- Findings: Thickened and swelling scrotal wall, perifascial hypoechoic fluid collection,
echogenic with dirty shadowing gas foci in scrotum.
- CT to assess the extent to retroperitoneum,
abdominal wall ...(3)
What we have to report?
- Localization: Epidermis/dermis,
fat,
muscle,
fascia,
joint...
- Size,
borders.
- Neighboring structures relationship.
- US characteristics (echogenicity,
solid/cyst,
Doppler signal...)
- To assess the feasibility of percutaneous treatment or FNA/CNB.
EMERGENCY IN SOFT TISSUE: 10 REASONS TO DO AN ULTRASOUND
- Every patient can undergo an US.
- 24 hours / 365 days availability.
- Bedside availability.
- As many times as necessary.
- Feasibility of therapeutic interventions.
- Wide and flexible field of view.
- Real-time dynamic examination.
- Differentiate solid vs cystic lesions.
- There is no ionizing radiation exposure.
- US is "cheap".
